
E-cigarette use is often discussed as a youth or young adult issue, but older adults should not be left out of the conversation. Smoking-related disease is highly concentrated in later life, and many older people who smoke have lived with decades of tobacco exposure. Understanding whether older adults use e-cigarettes, who uses them, and how vaping relates to smoking history and health status is therefore important for clinical care, tobacco control, and harm reduction.
Our new study, published in European Geriatric Medicine, examined the prevalence and correlates of current e-cigarette use among adults aged 60 years and over in Scotland.
Prevalence and correlates of e-cigarette use among older adults aged 60 years and over
Read Full Paper →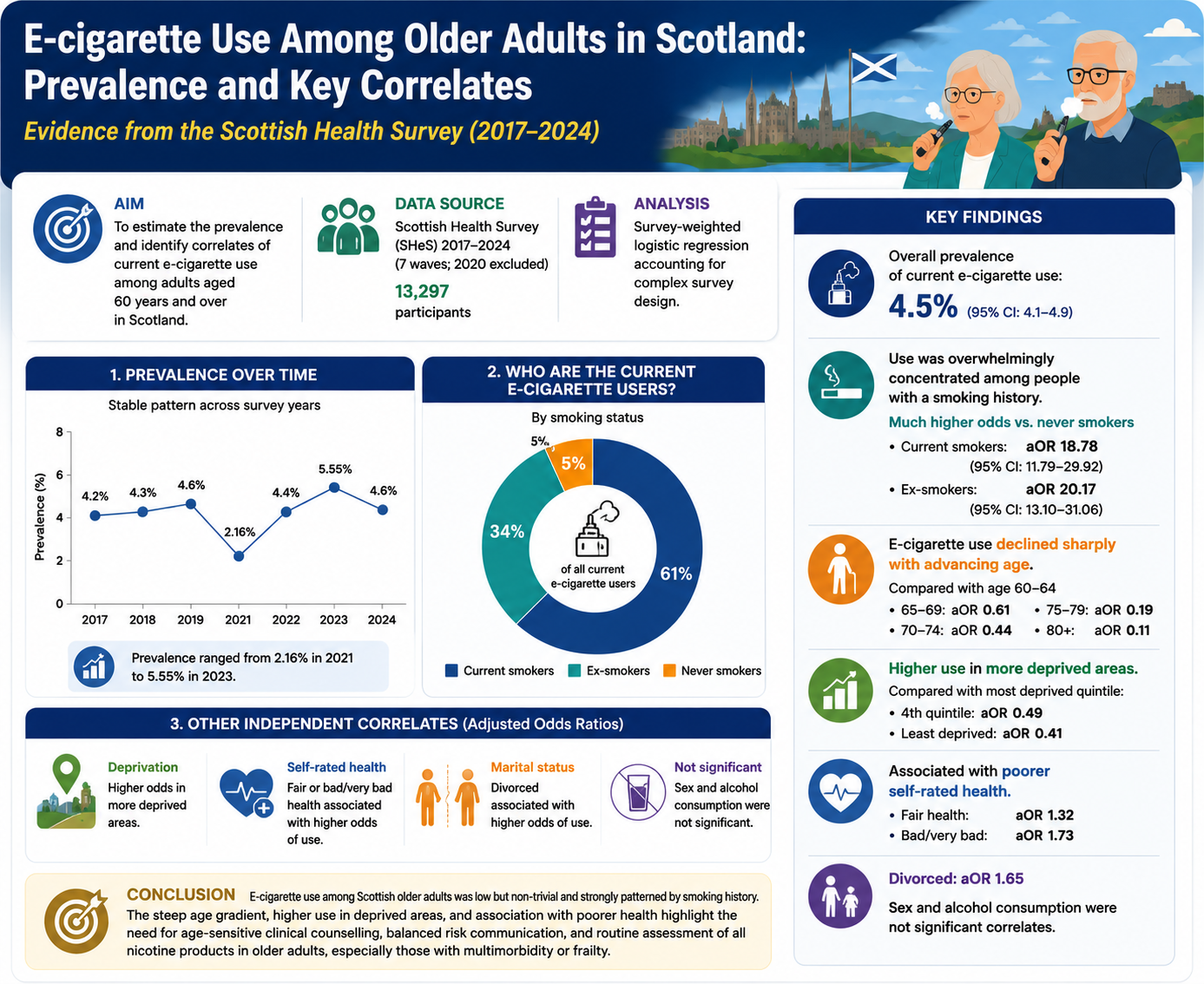
Why this study matters
Older adults carry a heavy burden of smoking-related illness, including cardiovascular disease, respiratory disease, cancer, frailty, and multimorbidity. Yet smoking cessation support is often less visible in older populations. Some older smokers may feel it is “too late” to quit, while healthcare professionals may focus more on existing conditions than on tobacco use.
This is a missed opportunity. Quitting smoking remains beneficial at older ages. E-cigarettes may be used by some older adults as a way to reduce or stop combustible cigarette use, but evidence on vaping in this age group is still limited.
Most studies of e-cigarette use focus on adolescents, young adults, or the general adult population. Our study focused specifically on older adults.
What we studied
We analysed data from 13,297 adults aged 60 years and over who participated in the Scottish Health Survey between 2017 and 2024, excluding 2020 because routine data collection was disrupted by the COVID-19 pandemic.
The Scottish Health Survey is a nationally representative household survey that collects information on health behaviours, smoking, vaping, alcohol use, deprivation, marital status, and self-rated health. The main outcome was current e-cigarette use. We examined how current vaping varied by age, sex, area deprivation, marital status, smoking status, alcohol consumption, self-rated health, and survey year.
What we found
Current e-cigarette use among older adults in Scotland was low but not negligible. The weighted prevalence was 4.5%.
Use was broadly stable across the study period, with some year-to-year fluctuation. The lowest estimate was observed in 2021, likely reflecting pandemic-related disruption, while estimates after 2021 returned to around 5%.
The strongest finding was the link with cigarette smoking history. E-cigarette use was overwhelmingly concentrated among current and former smokers. Only about 5% of current e-cigarette users had never smoked. This suggests that vaping among older adults in Scotland is mainly occurring among people with prior exposure to combustible tobacco, rather than representing widespread primary nicotine uptake among never smokers.
Compared with never smokers, current smokers and ex-smokers had much higher odds of current e-cigarette use. This was the dominant pattern in the study.
Only about 5% of current e-cigarette users had never smoked. Vaping among older adults in Scotland is mainly occurring among people with prior exposure to combustible tobacco, rather than representing widespread primary nicotine uptake among never smokers.
Age, deprivation, and health status mattered
E-cigarette use declined sharply with age. Adults aged 60–64 had the highest likelihood of current use, while those aged 80 and over had much lower odds. This may reflect generational differences, lower familiarity with vaping devices, functional barriers such as poor dexterity or eyesight, and different smoking histories among the oldest adults.
Vaping was also more common among older adults living in more deprived areas. This likely reflects the strong socioeconomic patterning of smoking itself, because smoking remains more common in disadvantaged communities. However, the deprivation pattern persisted even after adjustment, suggesting that social and economic circumstances may shape vaping behaviour among older adults.
Poorer self-rated health was also associated with current e-cigarette use. Older adults who rated their health as fair, bad, or very bad had higher odds of vaping than those reporting good or very good health. This does not mean vaping caused poorer health. The study was cross-sectional, so we cannot determine direction. It may be that older adults with smoking-related health problems switch to e-cigarettes after becoming unwell.
What the study cannot tell us
This study cannot determine why older adults use e-cigarettes. We could not tell whether vaping reflected smoking cessation, complete switching, experimentation, or ongoing dual use of both cigarettes and e-cigarettes.
The data also did not include details such as duration of vaping, nicotine strength, device type, quit intentions, pack-years, dependence severity, or timing of smoking cessation. These are important questions for future research.
What this means for clinical practice
Healthcare professionals should ask older adults about all nicotine product use, not just cigarette smoking. For older patients, especially those with frailty, multimorbidity, respiratory disease, cardiovascular disease, or poor self-rated health, clinicians should distinguish between complete smoking cessation, complete switching from smoking to vaping, and dual use.
The message should be balanced. E-cigarettes are not risk-free, but continued cigarette smoking is highly harmful. Older adults deserve clear, age-sensitive advice that reflects both the potential benefits of stopping combustible tobacco and the uncertainties around long-term vaping.
Bottom line
E-cigarette use among Scottish adults aged 60 and over was low but meaningful, and it was strongly concentrated among current and former smokers. Use declined with age, was higher in more deprived areas, and was associated with poorer self-rated health.
The findings highlight the need for routine nicotine-use assessment in older adults, better smoking cessation support in later life, and careful risk communication that avoids both alarmism and over-reassurance.

Comments
Loading comments...
Leave a Comment
Share your thoughts on this article.